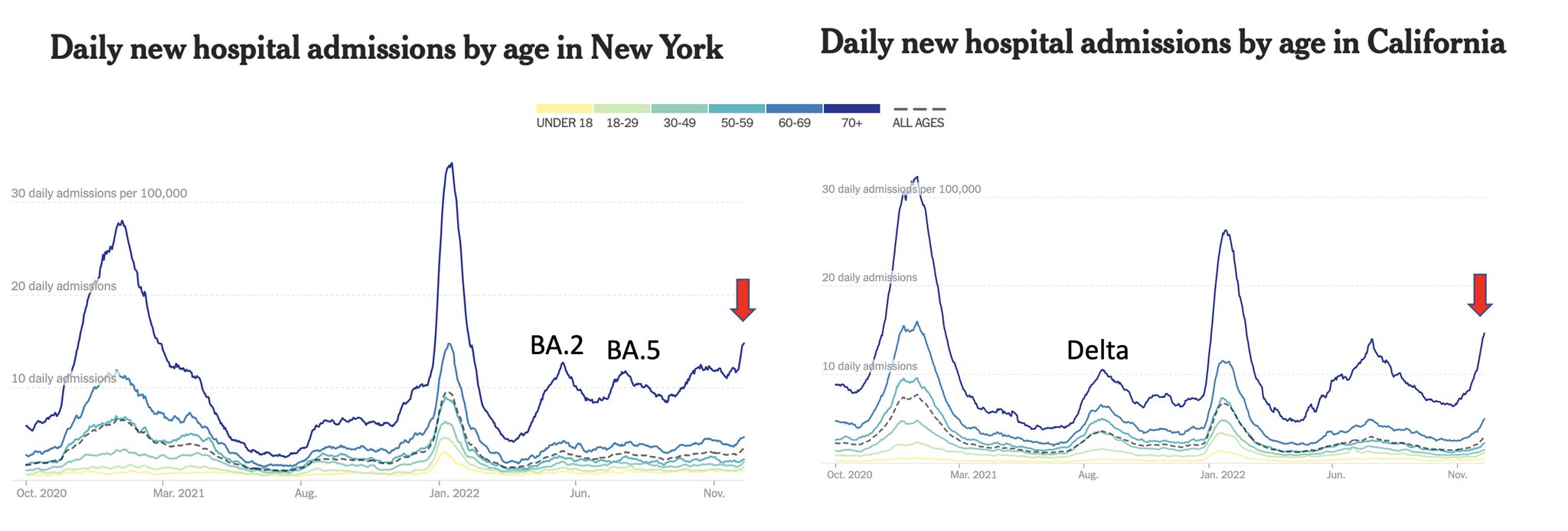
Over recent weeks, since before Thanksgiving, there has been a significant and steep rise in COVID-19-related hospitalizations for Americans 70 and older. Nationally, that rate now exceeds the peak of the BA.5 summer wave and the Delta wave in the summer of 2021 — and this surge is still in sharp ascent. This is a signal that we are in for some trouble.
The new wave is largely being missed, with scant media coverage. The case numbers, of about 50,000 per day, represent a gross underestimate because home rapid antigen tests are not centrally reported and because some people with symptoms or exposure are not getting tested. Nevertheless, tests of wastewater are finding levels of SARS-CoV-2 quickly rising, which tracks with the increase in hospitalizations among seniors. So does the rate of COVID test positivity, which has risen 35% in the past two weeks.
This is part of a global COVID wave, being seen throughout much of Europe, South America and the Middle East and in China, Japan, South Korea, Australia and New Zealand. The only continent that appears to be spared to date is Africa.
Why is this happening yet again, after 13 billion doses of vaccines have been administered and after more than 650 million confirmed infections? Shouldn’t enough people have enough immunity to stave off a wave of infections at this point? Unfortunately no, principally because our immune system protection against the virus wanes over time, especially as it evolved to Omicron and its multiple subvariants. By four to six months after vaccination or a booster shot, there is a substantial drop-off of neutralizing antibodies and protection against hospitalization — though that protection is largely restored by a new booster shot.
A second factor is that mitigation measures have largely been abandoned. Few people are masking, especially with N95 or KN95 masks, and there are more indoor gatherings occurring because of colder weather and the holidays. Testing is no longer as common to screen people who are exposed to the virus. Little to no attention is being paid to ventilation or air filtration. The pervasive attitude is that the pandemic is over.
It is not. Denial of circulating virus will not make it go away or reduce its toll of ill effects.
The third factor is the BQ.1.1 variant that is on a path to dominance. In the week ending Dec. 3, it constituted 32% of cases. This strain has an additional key mutation beyond BQ.1 that makes it more evasive of our immune system, so there is still more to expect of BQ.1.1’s impact as it continues to spread.
Notably, BQ.1.1 and another variant, XBB, are the two strains most effective at escaping our immune response, so effective that they resist all commercially available monoclonal antibodies and Evusheld, a combination antibody used to prevent the toll of infections in the immunocompromised.
So what can impede this growing wave? First, more people need to get the bivalent booster that is effective against Omicron variants. Only one in three seniors has had a booster over the past six months or longer; less than 15% of all Americans eligible have had the bivalent shot. In many peer countries the rate of recent boosters for seniors is 80% or higher. We are doing a pathetic job of protecting our elders here.
Newly posted data from the CDC show an 80% reduction of hospitalizations for people of all ages who had two booster shots compared with the unvaccinated. The bivalent booster, available since the first week in September, has shown a fivefold to tenfold increase in antibodies to BQ.1.1. This is fortunate; while we expected the booster would broaden the immune response to other variants, it was unknown whether it would help against BQ.1.1.
Second, mitigation factors — such as high-quality masks, distancing, testing and attention to air quality — should be used in places that pose a high risk of transmission. Anyone who doesn’t take seriously the risk of COVID infection is in denial about the risk of long COVID and its potentially disabling effects. And people should be taking precautions not only for their own sake but also out of respect for the immunocompromised and aged among us.
Now that vaccines and boosters don’t help reduce infection very much, or for very long, we have to go back to the basics for protection against respiratory viruses. That is not only a COVID precaution. Consider the high rate of influenza hospitalizations in the United States, the worst in the past decade, and RSV, which is also hitting children and older adults hard right now.
Beyond waning immunity and relaxed precautions, a third factor in this new wave is that we have failed to keep up with the virus. We’ve lost the powerful monoclonal antibodies as effective treatment backstops or for helping bolster protection for more than 7 million Americans who are immunocompromised. There are no backup pills yet to Paxlovid, which has been highly effective in reducing hospitalizations and deaths. Unlike other countries, the United States has shown no leadership for aggressively pursuing nasal vaccines, with their promise of blocking infections and transmission, or more durable, broadly effective, variant-proof vaccines.
We don’t know how severe the new COVID wave will be. With all the infections and vaccinations we’ve had here, there’s an immunity wall built that should reduce the severity of symptoms compared with some prior waves. But our relatively low rate of booster shots and our waned immunity leave the U.S. particularly vulnerable.
The new COVID wave is talking to us. Let’s listen and take action.
Eric J. Topol is a professor of molecular medicine at Scripps Research and author of the newsletter Ground Truths.
The new wave is largely being missed, with scant media coverage. The case numbers, of about 50,000 per day, represent a gross underestimate because home rapid antigen tests are not centrally reported and because some people with symptoms or exposure are not getting tested. Nevertheless, tests of wastewater are finding levels of SARS-CoV-2 quickly rising, which tracks with the increase in hospitalizations among seniors. So does the rate of COVID test positivity, which has risen 35% in the past two weeks.
This is part of a global COVID wave, being seen throughout much of Europe, South America and the Middle East and in China, Japan, South Korea, Australia and New Zealand. The only continent that appears to be spared to date is Africa.
Why is this happening yet again, after 13 billion doses of vaccines have been administered and after more than 650 million confirmed infections? Shouldn’t enough people have enough immunity to stave off a wave of infections at this point? Unfortunately no, principally because our immune system protection against the virus wanes over time, especially as it evolved to Omicron and its multiple subvariants. By four to six months after vaccination or a booster shot, there is a substantial drop-off of neutralizing antibodies and protection against hospitalization — though that protection is largely restored by a new booster shot.
A second factor is that mitigation measures have largely been abandoned. Few people are masking, especially with N95 or KN95 masks, and there are more indoor gatherings occurring because of colder weather and the holidays. Testing is no longer as common to screen people who are exposed to the virus. Little to no attention is being paid to ventilation or air filtration. The pervasive attitude is that the pandemic is over.
It is not. Denial of circulating virus will not make it go away or reduce its toll of ill effects.
The third factor is the BQ.1.1 variant that is on a path to dominance. In the week ending Dec. 3, it constituted 32% of cases. This strain has an additional key mutation beyond BQ.1 that makes it more evasive of our immune system, so there is still more to expect of BQ.1.1’s impact as it continues to spread.
Notably, BQ.1.1 and another variant, XBB, are the two strains most effective at escaping our immune response, so effective that they resist all commercially available monoclonal antibodies and Evusheld, a combination antibody used to prevent the toll of infections in the immunocompromised.
So what can impede this growing wave? First, more people need to get the bivalent booster that is effective against Omicron variants. Only one in three seniors has had a booster over the past six months or longer; less than 15% of all Americans eligible have had the bivalent shot. In many peer countries the rate of recent boosters for seniors is 80% or higher. We are doing a pathetic job of protecting our elders here.
Newly posted data from the CDC show an 80% reduction of hospitalizations for people of all ages who had two booster shots compared with the unvaccinated. The bivalent booster, available since the first week in September, has shown a fivefold to tenfold increase in antibodies to BQ.1.1. This is fortunate; while we expected the booster would broaden the immune response to other variants, it was unknown whether it would help against BQ.1.1.
Second, mitigation factors — such as high-quality masks, distancing, testing and attention to air quality — should be used in places that pose a high risk of transmission. Anyone who doesn’t take seriously the risk of COVID infection is in denial about the risk of long COVID and its potentially disabling effects. And people should be taking precautions not only for their own sake but also out of respect for the immunocompromised and aged among us.
Now that vaccines and boosters don’t help reduce infection very much, or for very long, we have to go back to the basics for protection against respiratory viruses. That is not only a COVID precaution. Consider the high rate of influenza hospitalizations in the United States, the worst in the past decade, and RSV, which is also hitting children and older adults hard right now.
Beyond waning immunity and relaxed precautions, a third factor in this new wave is that we have failed to keep up with the virus. We’ve lost the powerful monoclonal antibodies as effective treatment backstops or for helping bolster protection for more than 7 million Americans who are immunocompromised. There are no backup pills yet to Paxlovid, which has been highly effective in reducing hospitalizations and deaths. Unlike other countries, the United States has shown no leadership for aggressively pursuing nasal vaccines, with their promise of blocking infections and transmission, or more durable, broadly effective, variant-proof vaccines.
We don’t know how severe the new COVID wave will be. With all the infections and vaccinations we’ve had here, there’s an immunity wall built that should reduce the severity of symptoms compared with some prior waves. But our relatively low rate of booster shots and our waned immunity leave the U.S. particularly vulnerable.
The new COVID wave is talking to us. Let’s listen and take action.
Eric J. Topol is a professor of molecular medicine at Scripps Research and author of the newsletter Ground Truths.