I'll ask again, are you going to keep posting here or move over to the new on3 site? I want to be sure I am frequenting the board you intend to post on.I'm sure you don't understand any of it. Unsurprising


Colleges
- AAC
- ACC
- Big 12
- Big East
- Big Ten
- Pac-12
- SEC
- Atlantic 10
- Conference USA
- Independents
- Junior College
- Mountain West
- Sun Belt
- MAC
- More
- Navy
- UAB
- Tulsa
- UTSA
- Charlotte
- Florida Atlantic
- Temple
- Rice
- East Carolina
- USF
- SMU
- North Texas
- Tulane
- Memphis
- Miami
- Louisville
- Virginia
- Syracuse
- Wake Forest
- Duke
- Boston College
- Virginia Tech
- Georgia Tech
- Pittsburgh
- North Carolina
- North Carolina State
- Clemson
- Florida State
- Cincinnati
- BYU
- Houston
- Iowa State
- Kansas State
- Kansas
- Texas
- Oklahoma State
- TCU
- Texas Tech
- Baylor
- Oklahoma
- UCF
- West Virginia
- Wisconsin
- Penn State
- Ohio State
- Purdue
- Minnesota
- Iowa
- Nebraska
- Illinois
- Indiana
- Rutgers
- Michigan State
- Maryland
- Michigan
- Northwestern
- Arizona State
- Oregon State
- UCLA
- Colorado
- Stanford
- Oregon
- Arizona
- California
- Washington
- USC
- Utah
- Washington State
- Texas A&M
- Auburn
- Mississippi State
- Kentucky
- South Carolina
- Arkansas
- Florida
- Missouri
- Ole Miss
- Alabama
- LSU
- Georgia
- Vanderbilt
- Tennessee
- Louisiana Tech
- New Mexico State
- Middle Tennessee
- Western Kentucky
- UTEP
- Florida International University
High School
- West
- Midwest
- Northeast
- Southeast
- Other
- Alaska
- Arizona
- California
- Colorado
- Nevada
- New Mexico
- Northern California
- Oregon
- Southern California Preps
- Washington
- Edgy Tim
- Indiana
- Kansas
- Nebraska
- Iowa
- Michigan
- Minnesota
- Missouri
- Oklahoma Varsity
- Texas Basketball
- Texas
- Wisconsin
- Delaware
- Maryland
- New Jersey Basketball
- New Jersey
- New York City Basketball
- Ohio
- Pennsylvania
- Greater Cincinnati
- Virginia
- West Virginia Preps
ADVERTISEMENT
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
The coronavirus is speaking. It’s saying it’s not done with us.
- Thread starter Kenneth Griffin
- Start date
If Joe's Place wants it to speak he can spend about 30 posts telling us why it does.Anybody else shocked the the "Corona Virus can speak"? Seems like a earth shattering development to me.
No...it's a very common usage of the term. I'm shocked you've never heard it used before.Anybody else shocked the the "Corona Virus can speak"? Seems like a earth shattering development to me.
The real question is "would you want to have a beer with Corona Virus"?If Joe's Place wants it to speak he can spend about 30 posts telling us why it does.
I would.
Probably be hard to hold a conversation though. Every time a fatty would walk into the bar Corona would be distracted.
No...it's a very common usage of the term. I'm shocked you've never heard it used before.
FDA vaccine advisers 'disappointed' and 'angry' that early data about new Covid-19 booster shot wasn't presented for review last year | CNN
Some vaccine advisers to the federal government say they're "disappointed" and "angry" that government scientists and the pharmaceutical company Moderna didn't present a set of infection data on the company's new Covid-19 booster during meetings last year when the advisers discussed whether the...
In case you missed it... @GOHOX69Your studies seem to suggest that an early use of remdesivir in hospitalized patients with less than severe symptoms can be beneficial if minimal. The WHO study indicated:
Remdesivir has no significant effect on patients with COVID-19 who are already being ventilated. Among other hospitalised patients, it has a small effect against death or progression to ventilation (or both).
Your second link even says:
Remdesivir was the first antiviral to show clinical benefit in patients with moderate-to-severe COVID-19. Previous trials demonstrated a faster time to recovery in hospitalized patients treated with remdesivir vs placebo. Current guidelines recommend treatment with remdesivir based on hospitalization status, oxygen requirements, and time from symptom onset.
They don't refute that, so - apparently - they acknolwedge that it was effective but their paper is highly confusing and suffers from a very small sample size. Perhaps you can explain. They say:
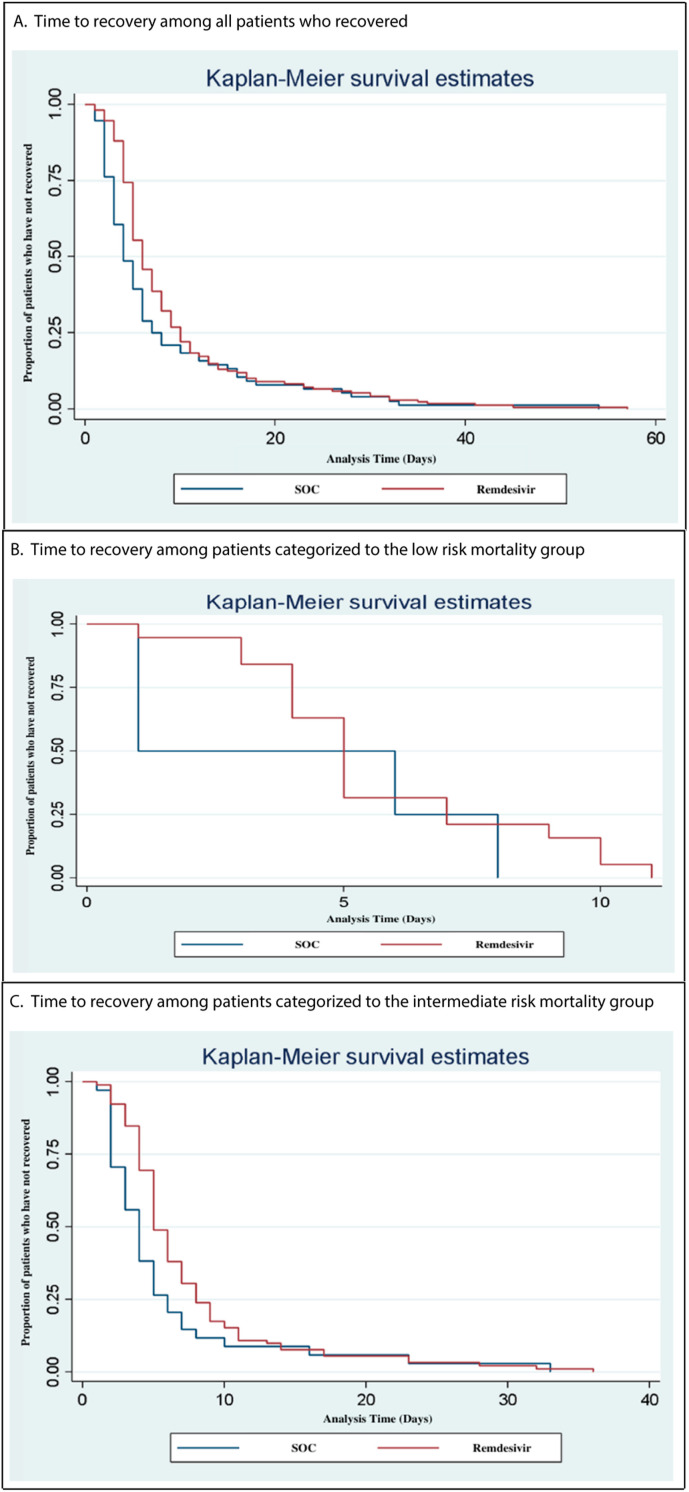
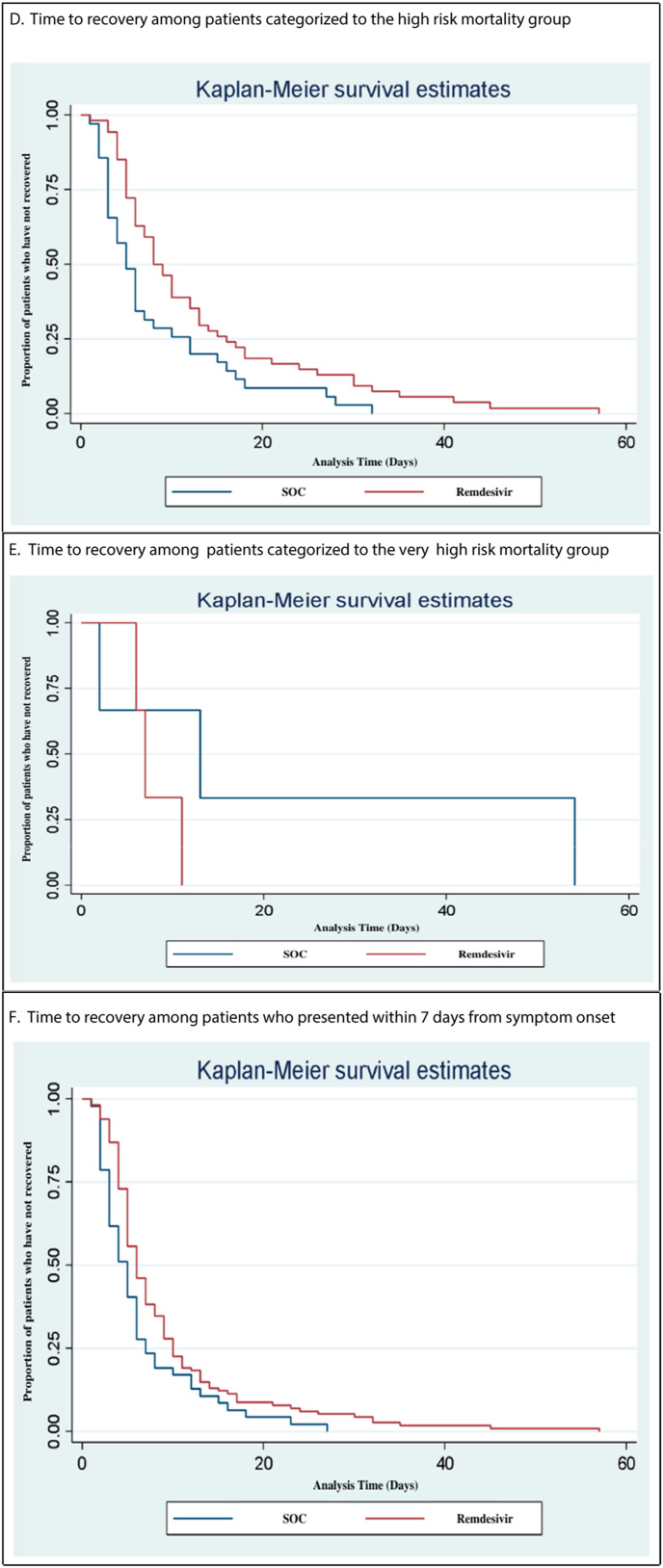
The primary outcome was time to recovery, defined as discharge from the hospital or no longer requiring supplemental oxygen, stratified by the 4C mortality score risk group. Secondary outcomes included in-hospital mortality, hospital length of stay, and time to recovery in patients who were started on remdesivir within 7 days from symptom onset vs after 7 days from symptom onset. A survival analysis was used to analyze time to recovery outcomes.
Fine..."Secondary outcomes included in-hospital mortality, hospital length of stay, and time to recovery in patients who were started on remdesivir within 7 days from symptom onset vs after 7 days from symptom onset". They address hospital length of stay. They address the difference in administration of remdesivir based on onset of symptoms. Could you show me where they address in-hospital mortality which would seem to be a big deal. Is that shown in the Survival Estimates somehow? If you could explain what Table B below is showing, that would be helpful.
And then perhaps explain how this gets it wrong, or doesn't:
Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients
CONCLUSIONS
Among nonhospitalized patients who were at high risk for Covid-19 progression, a 3-day course of remdesivir had an acceptable safety profile and resulted in an 87% lower risk of hospitalization or death than placebo.
It's a small sample size but the differences are stark.
I want to be sure I am frequenting the board you intend to post on.
He didn't miss it. He knows; he's just ignoring it.In case you missed it... @GOHOX69
He also ignored the two links to NIH and WHO policies regarding the administration of remdesivir for early-infections in high-risk patients. As already noted, it is not the first line of defense compared with easier-to-dose oral medications. But it is still on there as an option.In case you missed it... @GOHOX69
He cannot admit this and must carry on with his idiocy here.
EDIT: And the only thing they can reply with is laughy emojis. Sad.
Last edited:
More than just antivaxers. We know outcomes aren’t just dead/not dead. Vaccinated people are demonstrating organ damage at rates similar to non-vaccinated after covid infections. Imagine normalizing chronic health issues like dementia and heart failure in 40-50 year olds. This is the potential road the research shows we are headed down by letting this run wild. The signals are there. This is not a respiratory virus. It attacks your vasculature. The virus is found in brains post-mortem months after a mild infection. We will see if the research confirms it with time.Since the anti-vaxxers continue to ignore it, I'll re-post here:
CDC provisional data for 2022
Year Age Group COVID-19 Deaths Influenza Deaths Ratio 2022 Under 1 year 184 18 10.2 2022 0-17 years 606 130 4.7 2022 1-4 years 126 33 3.8 2022 5-14 years 183 67 2.7 2022 15-24 years 613 60 10.2 2022 18-29 years 1327 81 16.4 2022 25-34 years 2254 95 23.7 2022 30-39 years 3386 146 23.2 2022 35-44 years 4990 208 24.0 2022 40-49 years 7542 239 31.6 2022 45-54 years 11868 323 36.7 2022 50-64 years 37270 1069 34.9 2022 55-64 years 29913 861 34.7 2022 65-74 years 52000 1397 37.2 2022 75-84 years 65357 1770 36.9 2022 85 years and over 70845 1902 37.2
COVID:
- 5x more deaths in children, overall than flu
- 3x more in 5-14 yrs than flu
- 10x more in adolescents/young adults
- 16x-32x more in adults <50
- And the ratios go up from there....
COVID-19 Provisional Counts - Weekly Updates by Select Demographic and Geographic Characteristics
Tabulated data on provisional COVID-19 deaths by age, sex, race and Hispanic origin, and comorbidities. Also includes an index of state-level and county-level mortality data available for download.www.cdc.gov
I've highlighted what you said and it is 2000 percent correct. It's part of the imaging studies we are doing. It's not only post-mortem but it is insidious at activating genes that are responsible for Alzheimers. More on that laterMore than just antivaxers. We know outcomes aren’t just dead/not dead. Vaccinated people are demonstrating organ damage at rates similar to non-vaccinated after covid infections. Imagine normalizing chronic health issues like dementia and heart failure in 40-50 year olds. This is the potential road the research shows we are headed down by letting this run wild. The signals are there. This is not a respiratory virus. It attacks your vasculature. The virus is found in brains post-mortem months after a mild infection. We will see if the research confirms it with time.
")
In the immortal words of John Winger, It...Is...Alive...
https://aspr.hhs.gov/legal/PHE/Pages/covid19-11Jan23.aspx
https://aspr.hhs.gov/legal/PHE/Pages/covid19-11Jan23.aspx
More than just antivaxers. We know outcomes aren’t just dead/not dead. Vaccinated people are demonstrating organ damage at rates similar to non-vaccinated after covid infections. Imagine normalizing chronic health issues like dementia and heart failure in 40-50 year olds. This is the potential road the research shows we are headed down by letting this run wild. The signals are there. This is not a respiratory virus. It attacks your vasculature. The virus is found in brains post-mortem months after a mild infection. We will see if the research confirms it with time.
There are already a few studies indicating that vaccination is partly protective against Long Covid (and likely other sequelae that go with it).
Part of the issue is defining what "vaccinated" is now - 1 dose? 2? Bi-valent?
Because initial doses of the original vaccines are much less effective against the newer variants, and would suggest their protective effects will be lower.
So, comparing people who have had at least one dose + the bivalent against never-vaccinated and other partially vaccinated people (at least 3 groups) would be warranted, instead of lumping all people who have had "any" vaccine dose into a single group.
Terrifying. Are you using PET imaging?I've highlighted what you said and it is 2000 percent correct. It's part of the imaging studies we are doing. It's not only post-mortem but it is insidious at activating genes that are responsible for Alzheimers. More on that later
These studies can’t get published fast enough. The fact that we already had demonstrated differences two years into the pandemic is such a bad, bad sign.
We are using ultra resolution ct scanning. Molecular biology wise, we are using single cell transcriptomic sequencing.Terrifying. Are you using PET imaging?
These studies can’t get published fast enough. The fact that we already had demonstrated differences two years into the pandemic is such a bad, bad sign.
The studies I’ve read were pre-bivalent vaccines. They were mostly after the delta and first omicron surge. Vaccines were partially protective, but actually any infection is bad news for many organ systems.There are already a few studies indicating that vaccination is partly protective against Long Covid (and likely other sequelae that go with it).
Part of the issue is defining what "vaccinated" is now - 1 dose? 2? Bi-valent?
Because initial doses of the original vaccines are much less effective against the newer variants, and would suggest their protective effects will be lower.
So, comparing people who have had at least one dose + the bivalent against never-vaccinated and other partially vaccinated people (at least 3 groups) would be warranted, instead of lumping all people who have had "any" vaccine dose into a single group.
Keep in mind these changes are likely subclinical in many - it’s not just death/long covid - though those are definitely higher on the list to prevent. The issue with subclinical changes is they add up over time. It’s kind of like using pack years to assess your risks from smoking.
Far beyond my understanding. Thanks for the insights and your work. Look forward to reading the research (but maybe not actually).We are using ultra resolution ct scanning. Molecular biology wise, we are using single cell transcriptomic sequencing.
What the preliminary data shows is that Sars-Cov-2 infections activate some of the genes involved in the initiation of Alzheimer's Disease.Far beyond my understanding. Thanks for the insights and your work. Look forward to reading the research (but maybe not actually).
We have also seen many many micro clots both in the brain and pulmonary vasculature.
Other groups have reported similar findings.

Association of COVID-19 with New-Onset Alzheimer's Disease - PubMed
An infectious etiology of Alzheimer's disease has been postulated for decades. It remains unknown whether SARS-CoV-2 viral infection is associated with increased risk for Alzheimer's disease. In this retrospective cohort study of 6,245,282 older adults (age ≥65 years) who had medical encounters betw …
 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov
@GOHOX69 - I'm truly curious. I wasn't anything but respectful in my request, as far as I can tell. You published studies that I found confusing...particularly the graphs that were part of the study that documented longer hospital stays for those treated with remdesivir.
https://pubmed.ncbi.nlm.nih.gov/36603741/
It appears to me that they did a retrospective of patients who had already been discharged. That indicates that they started with people who had survived but it doesn't seem to take into account what percentage of patients initially admitted made it that far - which, it would seem, would have to be accounted for to make their results relevant..
Data was collected and analyzed for a total of 300 patients, of which 200 received remdesivir and 100 received SOC.
That, by itself, doesn't tell us anything about the actual effectiveness of the treatment.
Hypothetical...
They start with 800 patients admitted. They divide them into two groups of 400 - one group is treated with remdesivir, one group gets SOC. Now we get to their numbers...200 of those receiving remdesivir survived to be discharged while only 100 of those who received SOC survived. The authors may account for that somewhere which is why I asked but if they didn't then...frankly, I don't give a damn if I spend a few extra days in the hospital if it means I have double the chance of surviving in the first place.
So...I'll ask again. Can you address that particular study in any substantive way or do I get another "Like"?
https://pubmed.ncbi.nlm.nih.gov/36603741/
It appears to me that they did a retrospective of patients who had already been discharged. That indicates that they started with people who had survived but it doesn't seem to take into account what percentage of patients initially admitted made it that far - which, it would seem, would have to be accounted for to make their results relevant..
Data was collected and analyzed for a total of 300 patients, of which 200 received remdesivir and 100 received SOC.
That, by itself, doesn't tell us anything about the actual effectiveness of the treatment.
Hypothetical...
They start with 800 patients admitted. They divide them into two groups of 400 - one group is treated with remdesivir, one group gets SOC. Now we get to their numbers...200 of those receiving remdesivir survived to be discharged while only 100 of those who received SOC survived. The authors may account for that somewhere which is why I asked but if they didn't then...frankly, I don't give a damn if I spend a few extra days in the hospital if it means I have double the chance of surviving in the first place.
So...I'll ask again. Can you address that particular study in any substantive way or do I get another "Like"?
@GOHOX69 ...I gave you credit that was apparently misplaced. Duly noted.
@GOHOX69 - I'm truly curious. I wasn't anything but respectful in my request, as far as I can tell. You published studies that I found confusing...particularly the graphs that were part of the study that documented longer hospital stays for those treated with remdesivir.
https://pubmed.ncbi.nlm.nih.gov/36603741/
It appears to me that they did a retrospective of patients who had already been discharged. That indicates that they started with people who had survived but it doesn't seem to take into account what percentage of patients initially admitted made it that far - which, it would seem, would have to be accounted for to make their results relevant..
Data was collected and analyzed for a total of 300 patients, of which 200 received remdesivir and 100 received SOC.
That, by itself, doesn't tell us anything about the actual effectiveness of the treatment.
Hypothetical...
They start with 800 patients admitted. They divide them into two groups of 400 - one group is treated with remdesivir, one group gets SOC. Now we get to their numbers...200 of those receiving remdesivir survived to be discharged while only 100 of those who received SOC survived. The authors may account for that somewhere which is why I asked but if they didn't then...frankly, I don't give a damn if I spend a few extra days in the hospital if it means I have double the chance of surviving in the first place.
So...I'll ask again. Can you address that particular study in any substantive way or do I get another "Like"?
remdesivir | This Week in Virology
www.microbe.tv
These researchers do a good job breaking down recent scientific studies for all viral issues in terms easy to understand for the general public. Feel free to listen to one of their many podcasts that include findings for remdesivir. Or don’t… and expect someone’s valuable time and knowledge to be wasted on an anonymous unchangeable mind.
I simply asked @GOHOX69 to explain an issue with the papers he posted. I think I did so in a respectful manner. If you feel the need to go to bat for him since he seems unable to explain HIS posts, you can start there. Or don’t. Just don’t waste my “valuable time”. 😂remdesivir | This Week in Virology
www.microbe.tv
These researchers do a good job breaking down recent scientific studies for all viral issues in terms easy to understand for the general public. Feel free to listen to one of their many podcasts that include findings for remdesivir. Or don’t… and expect someone’s valuable time and knowledge to be wasted on an anonymous unchangeable mind.
Perhaps you should just ‘trust the science’, instead of ‘doing your own research’.I simply asked @GOHOX69 to explain an issue with the papers he posted. I think I did so in a respectful manner. If you feel the need to go to bat for him since he seems unable to explain HIS posts, you can start there. Or don’t. Just don’t waste my “valuable time”. 😂
I mean, I read your question and I still have no idea what you were asking. You have issue with the design of the study? Medicine is imperfect. You don’t understand why they chose the endpoints they did? The paper was looking at length of stay, it reported other outcomes but that is not what the study was designed to look at.I simply asked @GOHOX69 to explain an issue with the papers he posted. I think I did so in a respectful manner. If you feel the need to go to bat for him since he seems unable to explain HIS posts, you can start there. Or don’t. Just don’t waste my “valuable time”. 😂
I don’t know your background but I assume it’s not in medicine. It’s hard to teach someone how to evaluate medical literature critically and understand it. It’s frankly a waste of time to do it online, especially if someone is just being a contrarian asshole (not saying you are, but maybe you are).
Lol…if you can’t understand a very simple question, I can’t help you. It’s not about the end point they chose, it’s about the STARTING point they chose. Why don’t you tell @GOHOX to pull on his big boy pants and explain the paper he chose to post which purportedly is trying to make a point but seems to fail.I mean, I read your question and I still have no idea what you were asking. You have issue with the design of the study? Medicine is imperfect. You don’t understand why they chose the endpoints they did? The paper was looking at length of stay, it reported other outcomes but that is not what the study was designed to look at.
I don’t know your background but I assume it’s not in medicine. It’s hard to teach someone how to evaluate medical literature critically and understand it. It’s frankly a waste of time to do it online, especially if someone is just being a contrarian asshole (not saying you are, but maybe you are).
Last edited:
Lol…when you’re getting backed by this guy, @GOHOX69…you should reevaluate your life choices. Seriously.Perhaps you should just ‘trust the science’, instead of ‘doing your own research’.
He's asking GOHOX to explain his statements that "remdesivir doesn't work" and "is not recommended by WHO", when the evidence clearly indicates otherwise. And it's been linked multiple times.I mean, I read your question and I still have no idea what you were asking.
GOHOX merely cited literature that it doesn't work in people with severe cases, already hospitalized (this has been known for well over a year, that the antivirals are only useful early on in the infection period, and corticosteroids are necessary after the disease has progressed, to calm down the immune system).
Remdesivir IS being used for high-risk patients BEFORE they are hospitalized with success. And current guidelines by both WHO and NIH still list it as an option (below the oral meds, which are much easier to administrate). It is no longer the primary option, but if it is all you have available, it is better than nothing for early infections.
GOHOX also made a silly claim about "not being able to follow up on adverse events" using IV-administrated therapies, which is total nonsense. Outpatient IV treatments are routinely monitored for adverse events (e.g. chemotherapy). With things like "follow-up" and communication methods like "phones".
IV treatments are certainly inferior to the ease of oral meds, but no one is arguing this point here.
“(this has been known for well over a year, that the antivirals are only useful early on in the infection period, and corticosteroids are necessary after the disease has progressed, to calm down the immune system).”He's asking GOHOX to explain his statements that "remdesivir doesn't work" and "is not recommended by WHO", when the evidence clearly indicates otherwise. And it's been linked multiple times.
GOHOX merely cited literature that it doesn't work in people with severe cases, already hospitalized (this has been known for well over a year, that the antivirals are only useful early on in the infection period, and corticosteroids are necessary after the disease has progressed, to calm down the immune system).
Remdesivir IS being used for high-risk patients BEFORE they are hospitalized with success. And current guidelines by both WHO and NIH still list it as an option (below the oral meds, which are much easier to administrate). It is no longer the primary option, but if it is all you have available, it is better than nothing for early infections.
GOHOX also made a silly claim about "not being able to follow up on adverse events" using IV-administrated therapies, which is total nonsense. Outpatient IV treatments are routinely monitored for adverse events (e.g. chemotherapy). With things like "follow-up" and communication methods like "phones".
IV treatments are certainly inferior to the ease of oral meds, but no one is arguing this point here.
This is a really interesting take because in August last year, you and the ultra-ignorant 33 were on here arguing with me about the positive results of RVD with inpatient care. With you jumping on board with 33 that without RVD there would have been more deaths despite ZERO evidence to that fact. NOW you’re admitting it doesn’t work within the hospital setting, yet RVD is STILL the standard of care for inpatients. Care to explain that little nugget? Care to explain how RVD was approved for use for covid? I’d love to hear all the “evidence” of it working and how it got approved by the FDA without even going through their advisory board.
And isn’t it a wonder that the ONLY early treatment RCT done on RVD had absolutely wonderful results! Let’s see who did the study which was based on SURVEY results? None other than the drug maker itself, Gilead! Oh, and the trial was “terminated early due to administrative issues”. Nothing to see there. BTW the WHO DID recommend against RVD based upon their own trial that showed it was worthless with inpatient. It only recommended it again from this ONE RCT on early treatment.
Really?“(this has been known for well over a year, that the antivirals are only useful early on in the infection period, and corticosteroids are necessary after the disease has progressed, to calm down the immune system).”
This is a really interesting take because in August last year, you and the ultra-ignorant 33 were on here arguing with me about the positive results of RVD with inpatient care.
I cited peer reviewed references. And I pointed out the pill form would be superior, when it was still being cited by it's experimental name. WAY before you even knew what "remdesivir" was....
“(this has been known for well over a year, that the antivirals are only useful early on in the infection period, and corticosteroids are necessary after the disease has progressed, to calm down the immune system).”
This is a really interesting take because in August last year, you and the ultra-ignorant 33 were on here arguing with me about the positive results of RVD with inpatient care. With you jumping on board with 33 that without RVD there would have been more deaths despite ZERO evidence to that fact. NOW you’re admitting it doesn’t work within the hospital setting, yet RVD is STILL the standard of care for inpatients. Care to explain that little nugget? Care to explain how RVD was approved for use for covid? I’d love to hear all the “evidence” of it working and how it got approved by the FDA without even going through their advisory board.
And isn’t it a wonder that the ONLY early treatment RCT done on RVD had absolutely wonderful results! Let’s see who did the study which was based on SURVEY results? None other than the drug maker itself, Gilead! Oh, and the trial was “terminated early due to administrative issues”. Nothing to see there. BTW the WHO DID recommend against RVD based upon their own trial that showed it was worthless with inpatient. It only recommended it again from this ONE RCT on early treatment.
I posted on the oral medication version clinical trial barely 2 months into the pandemic:
Orlando Health doctor says they have used convalescent plasma in 12 patients with "great results"
Orlando Health doctor says they have used convalescent plasma in 12 patients and are seeing great results From CNN’s Jamiel Lynch Physicians at Orlando Health have used convalescent plasma transplants in 12 patients and are seeing great results, Dr. Sunil Desai said in a press conference...
 iowa.forums.rivals.com
iowa.forums.rivals.com
EIDD-2801
EIDD-2801
FDA Clears the Way for Ridgeback Biotherapeutics to begin Human Testing of a Promising Potential Treatment for COVID-19 4/7/2020 EIDD-2801, an oral broad-spectrum antiviral proceeding into Clinical Trials ATLANTA and MIAMI, April 6, 2020 /PRNewswire/ -- Ridgeback Biotherapeutics LP, a closely...
iowa.forums.rivals.com

I see the usual suspect has returned.
You still denying these anti-virals work? They are all still recommended by WHO, NIH and most healthcare professionals. There are actual MDs on this site who post Likes to my post about them; you seem to be a bit behind the curve here.
Similar threads
- Replies
- 13
- Views
- 486
- Replies
- 6
- Views
- 173
- Replies
- 0
- Views
- 103
ADVERTISEMENT
Latest posts
-
-
-
 Missouri State Transfer WR Raylen Sharpe Visiting Iowa on Tuesday
Missouri State Transfer WR Raylen Sharpe Visiting Iowa on Tuesday- Latest: Eliot Clough
-
-

ADVERTISEMENT