Presumably their methodology did not change, yet the deaths dropped dramatically.
Your bias is making you blind.
The COVID-19 death toll has been four times higher in lower-income countries than in rich ones, according to a new report published today by Oxfam on behalf of the People’s Vaccine Alliance as the world marks two years since the World Health Organization declared the pandemic.
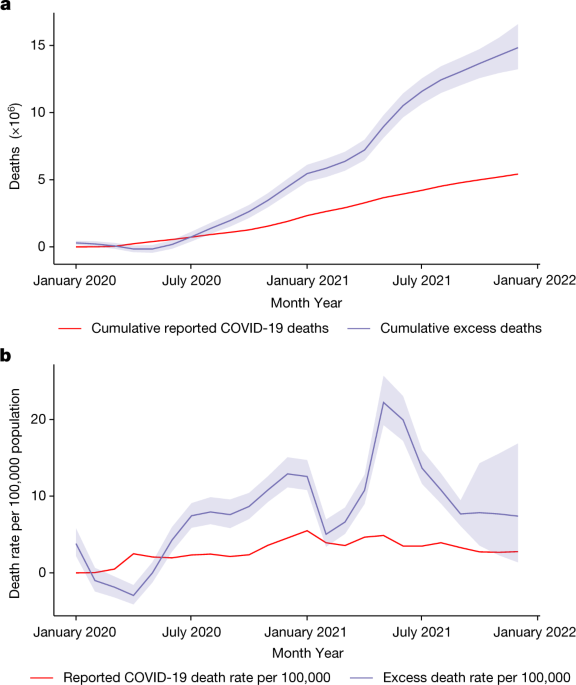
While the pandemic has been devastating for rich countries like the US and the UK, the world’s poorest countries have been hardest hit, with women and children bearing a disproportionate burden. Lack of testing and reporting means that very large numbers of deaths due to COVID-19 go unreported, especially in the poorest countries. Modelling using measures of excess deaths estimates that 19.6 million people have died because of COVID-19, over three times the official death toll. Based on this analysis, Oxfam calculated that for every death in a high-income country, an estimated four other people have died in a low or lower-middle income country. On a per capita basis, deaths in low and lower middle-income countries are 31 percent higher than high income countries.