Ohh boy soo much to unpack here and def game me a laugh .... it really goes to show the #dunningkruger effect in full force....lets just unpack your post ... i have 15 min before I need to get going.
NIH acknowledging renal failure as an adverse side effect? Liver damage??!!! Yep
Review this table to learn about the characteristics of drugs under study for the treatment of COVID-19.
www.covid19treatmentguidelines.nih.gov
Lol the CYA from the NIH.... liver enzymes may go up....but do you know what goes up in viral infections?? I'll save you the time, its AST/ALTs.
As for them listing renal/Liver failure. The direct quote "Drug vehicle is SBECD, which has been associated with renal and liver toxicity." I hope you arent basing your renal failure on this part. SBECD can cause liver/renal and other issues....but at doses much much higher and longer than what would be given with RDV. SBECD isn't something new to manage. For a 5-10 day course there is no risk of accumulation to occur.
Continue to educate yourself
Introduction Intravenous (IV) voriconazole is not recommended in patients with creatinine clearance <50 ml/min to avoid potentially toxic accumulation of sulfobutylether-β-cyclodextrin (SBECD). The purpose of this study was to evaluate the pharmacokinetics of SBECD, voriconazole, and...
ccforum.biomedcentral.com
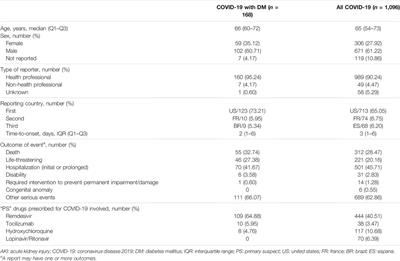
Wonderful study here showing serious adverse events and renal failure? Yep. But you've never heard of it huh?
https://www.nejm.org/doi/full/10.1056/NEJMoa2007016 "A total of 32 patients (60%) reported adverse events during follow-up (
Table 2). The most common adverse events were increased hepatic enzymes, diarrhea, rash, renal impairment, and hypotension. In general, adverse events were more common in patients receiving invasive ventilation. A total of 12 patients (23%) had serious adverse events. The most common serious adverse events — multiple-organ-dysfunction syndrome, septic shock, acute kidney injury, and hypotension — were reported in patients who were receiving invasive ventilation at baseline"
What were those rates in control group?? ohh no control group...and all the adverse events have in the vent group?? Well here is something else for you to learn. Ppl on vents tend to have have bad outcomes including but not limited to organ injury....tends to happen right after vent as well...you know since ppl usually are pretty hypoxic prior to vent .... and organs being hypo perfused is not a good outcome. Take it one step further and these patients also tend to need pressor support as well....well that pressure support can cause the arteries in the kidney to "clamp" down and thus cause more AKI
Continue to educate yourself
Mechanical ventilation is associated with significant increases in the risk of acute kidney injury (AKI). The rate of AKI due to mechanical ventilation and the associated mortality remain unacceptably high. Preventative and therapeutic strategies are ...

www.ncbi.nlm.nih.gov
WHO recommended against it until gasp some new "study" came out in April 2022 (treatment not hospitalization)

www.who.int
A better question is why the WHO sat on a trial for >1 .... that showed decreased mortality...
lol "studies" Its a computer search looking key words...using a data system .... no control group what so ever and pulling certain terms.... yeah one could reasonably say they need to look at this data in a RCT to see if holds up but only a true #dunningkruger would think this is a gotcha moment.
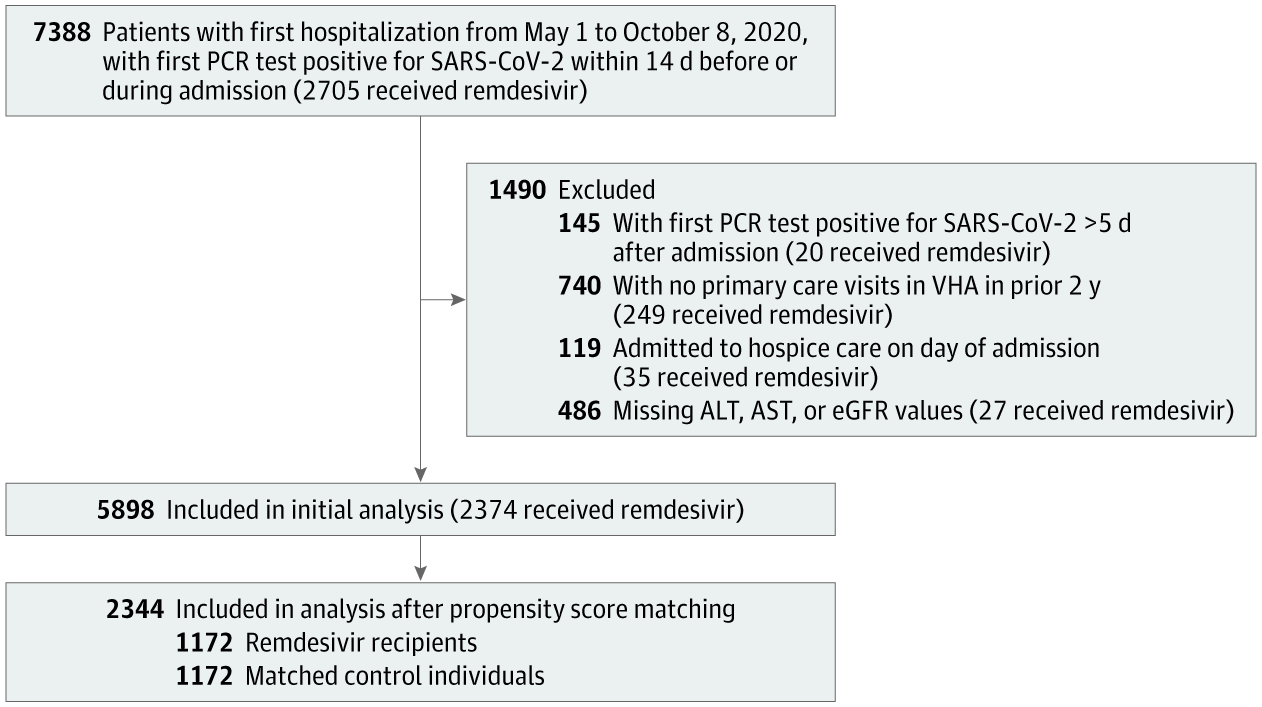
Even our own University of Iowa published a study of how lousy the drug is
In true #dunningkruger fashion you want to compare a retrospective/observational cohort to a meta-analysis (filled with quality RCTs)?? Yes that data should lead you to want to complete a RCT but to say it has any meaning against RCT and specifically a meta-analaysis??? Thats not how it work....
It's a wonder why Fauci, without any verifiable evidence in 2020 (he used a study that changed it's outcome from mortality to reduced hospital stay in the middle of the study), put this crappy drug approved to be used in the hospital setting and has the audacity to give hospitals a 20% bonus payment for using under CMS changes? Could it be his old buddy Ralph Baric, infamous for his connection to Wuhan and gain-of-function research, was part of making this drug? Nah, you wouldn't pay ANY attention to these conflicts of interest would you?
without even getting into your brand of crazy and going off the rails here...but...lets just "pretend" everything you said is true (which so far nothing you have said is true)...but lets pretend...how does this have any effect on the data the meta-analysis showed?? well it doesn't...and doesn't change results of the data
Let's next tackle your little meta-analysis horseshit you sent over (taking aside your smart ass, inconsequential Bayesian mathematics stupidity). There have only been 8 RCTs for remdesivir for Covid.
You do realize in all your dunningkruger glory that meta-analysis are superior to RCT ..... well as long as they are conducted correctly and use good studies to make up the meta... if you fill a meta with crap studies ...you will get crap results which we can look at later.
- 1 Early treatment study showing AMAZING results that you touted funded by none other than Gilead! You know the maker of Remdesivir. How convenient for the narrative!
Its not like they are hiding that they funded it....but maybe your should look up the Idaho VA home and see the logical progession to why they wanted fund this trial. You know its ok for a drug company to do a trial right?? Especially if its clearly known.... can you tell me the biases them funding the trial created??
7 late treatment studies, 2 of which show negative benefits, 3 showing little to no benefit (including the largest trial showing this wonderful outcome: Death occurred in 301 of 2743 patients receiving remdesivir and in 303 of 2708 receiving its control) and 2 showing marginal benefit.
again a meta-analysis can show benefit comprised from only studies that showed none...and would be considered higher quality evidence than any of those RCTs that comprise the meta. At this time you will need to explain that the quality of evidence used in the meta is not good .... otherwise using data from RCTs in the meta against the meta is a sure fire #krugerdunning move.
But by all means tout that magnificent turd of a meta analysis while completely discounting the 2 meta's done on IVM because it doesn't fit your narrative.
fill a meta with crap...and you get crap in return...but here is another recently published gem
If remdesivir was so effective we would have had much less deaths around the world.
Lol, or one could say without remdesivir there would have been much more deaths..... a #dunningkruger statement at its finest.
A drug made for ebola and it had a worse death rate than the disease itself and was pulled from the study
I know we know this...but i dont think you know how to read and understand studies well....
But by all means, smart guy, keep injecting a drug that has no anti-inflammatory qualities during the pulmonary inflammation stage.
ohh by all means please tell use when the viremic stage completely ends and is all inflammatory stage.... you understand they overlap for quite a bit?? Like pry why the last 2 meta-analysis have showed remdesivr benefit prior to vent....also never used in vent patients ... and very few ppl i know have either...maybe during the compassionate use days but its not like it was wide spread.
You're an idiot and should have been encouraging early treatment instead of this crap when patients came into the hospital
I have always advocated for early treatment you know like the vaccine...wearing a mask and trying to get into better shape/health
I'm not answering anymore because your arguments SUCK.
No, you arent answering anymore because you are truly an idiot that thinks they know something of a subject when you clearly don't. you are the poster child for #dunningkruger



 pubmed.ncbi.nlm.nih.gov
pubmed.ncbi.nlm.nih.gov